Venous Thrombo Embolism (VTE) is a common, lethal disorder affecting hospitalized and non-hospitalized patients. Often overlooked, it recurs frequently and results in long-term complications. VTE consists of Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE).
VTE is one of the most common cardiovascular illnesses, third only to acute coronary syndrome and stroke.* It contributes substantially to patient morbidity, mortality and cost of management.
The true incidence of VTE is hard to estimate. Here are some startling statistics:
- Average annual incidence of VTE among whites is 108 per 100,000 person years with about 250,000 incident cases occurring annually among US whites.**
- A study spanning 19 Asian countries revealed that DVT occurred in 41% of patients undergoing major hip joint surgery without thrombo-prophylaxis. ***
- In another global epidemiological study consisting of 68,183 patients including 2,058 from India, 52% (55% medical and 45% surgical) were found at risk of developing VTE. In that study, 54% of hospitalized (45% medical and 61% surgical) Indian patients had risk factor for VTE.
- In one retrospective study, the incidence of VTE is reported to be 28% in south Indian population.
- The overall incidence of PE in adult medical autopsies was 15.9% (159/1,000) in a study from a tertiary care hospital in Northern India which also reported an incidence of 79.87% in younger population; those below the age of 50 years.
Testing Scenario in India
D Dimer testing is of clinical use when there is a suspicion of VTE and is nowadays a commonly referred test. Unfortunately, not many laboratories in India can perform these tests due to limitations of manual systems. Most of the estimated 40,000 clinical laboratories in India still do not have this testing facility due to financial constraints, demographic challenges, non - availability of reliable tests kits and trained expertise.
Different D Dimer Assays
There are multiple technologies available for D Dimer testing. However, not all are specific, sensitive, quantitative and at the same time affordable. Another limitation is that these kits are often available in large pack sizes, with reagents of limited expiry. As a result, a lot of prospect centres, with a small workload, postpone the procurement decision.
Comparison of various methods of D Dimer Assay
Comparison of various methods of D Dimer Assay
| Method |
Sample Type |
Sensitivity |
Specificity |
Calibration required |
QC possible |
System required |
Remarks |
| Microplate ELISA |
Plasma |
High |
Low |
Yes |
Yes. L-J possible |
Manual |
Long procedure with ELISA readers |
| Fluorescence Immuno Assay/ ELFA |
Plasma |
High |
Low |
Yes |
Yes. L-J possible |
Automated |
Costly FIA system |
| Chemilumescence Systems |
Plasma |
High |
Low |
Yes |
Yes. L-J possible |
Automated |
Costly CLIA system |
| Immunofilteration and Sandwich type Systems |
Plasma |
High |
Low-High |
No |
No |
Automated |
Low specificity for boronate method |
| Semi Quantitative Latex agglutination slide tests |
Plasma |
Moderate |
Moderate |
No |
Basic |
Manual |
Outdated slide test, manual |
| Manual Whole Blood agglutination Rapid test |
Whole Blood |
High-Moderate |
Moderate |
No |
Basic |
Manual |
Kits not easily available |
| Second Generation Latex Agglutination Test |
Plasma |
High |
Moderate |
Yes |
Yes. L-J possible |
Automated |
Possible only on fully automated system |
Latex Based Testing of D Dimer
Latex Based is the most common for D Dimer testing kits. However, the type and size of latex, matters a lot. The light-scattering properties of micro-particles depend mainly on two variables: the size of the particles and the wavelength of the light. A small particle would not work well at long wavelengths, whereas a large particle would behave poorly at shorter wavelengths. Most of the analyzers available have the wavelength of 405 nm as an option. Smaller semi-automatic coagulation analyzers may have 405 nm as the only option. Almost all D Dimer kits are designed for these analyzers. However all these kits suffer from interferences such as, hemoglobin, bilirubin and lipids are present. At low wavelength, such as 405 nm, the absorbance from these interfering substances is very high.
D Dimer R operates at higher wavelengths, typically around 800 nm, where there is no effect of interfering substances. ECL series Coagulation analyzers are capable to run these specialized, advanced D Dimer reagents.
Calibration
D Dimer tests are reported in DDU or ng/ml FEU units.
The calibration curve is made with a dedicated calibrator, with serial dilution to 1/32.
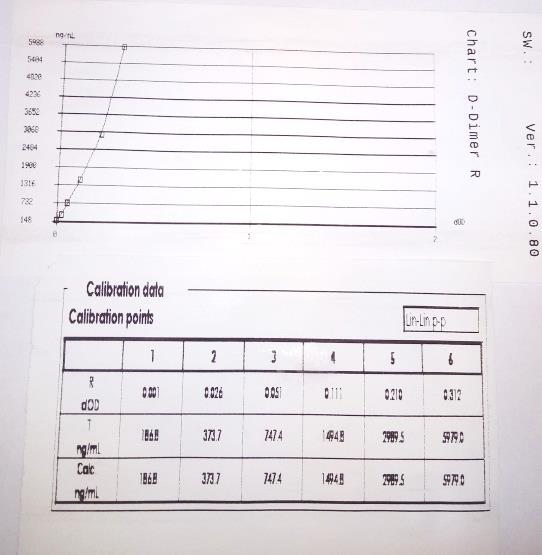 Fig. Typical D-Dimer R Calibration Curve
Fig. Typical D-Dimer R Calibration Curve
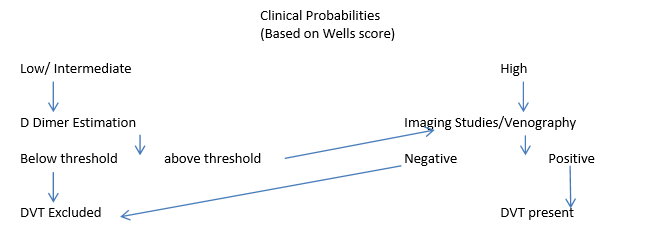
Clinical Probabilities
Wells Criteria
Wells Criteria for DVT
| Clinical feature |
Points |
| High probability |
3 or greater |
| Moderate probability |
1 or 2 |
| Low probability |
0 or less |
| Active cancer |
1 |
| Paralysis, paresis or recent plaster immobilisation of the extremities |
1 |
| Recently bedridden for more than 3 days within the last 4 weeks |
1 |
| Localised tenderness along the distribution of the venous system |
1 |
| Entire leg swollen |
1 |
| Calf swelling by more than 3 cm when compared to the asymptomatic leg (measured below tibial tuberosity) |
1 |
| Pitting oedema (greater in symptomatic leg) |
1 |
| Collateral superficial veins (non-varicose) |
1 |
| Alternative diagnosis as or more likely than that of DVT |
-2 |
Wells criteria for pulmonary embolism
| Clinical feature |
Points |
| High probability |
6 or greater |
| Moderate probability |
2.0 to 6.0 |
| Low probability |
Less than 2.0 |
| Clinical symptoms of DVT (leg swelling, pain on palpitation) |
3.0 |
| Other diagnosis less likely than pulmonary embolism |
3.0 |
| Heart rate>100 |
1.5 |
| Immobilisation (>/= 3 days) or surgery in the previous 4 weeks |
1.5 |
| Previous DVT/PE |
1.5 |
| Haemoptysis |
1.0 |
| Malignancy |
1.0 |
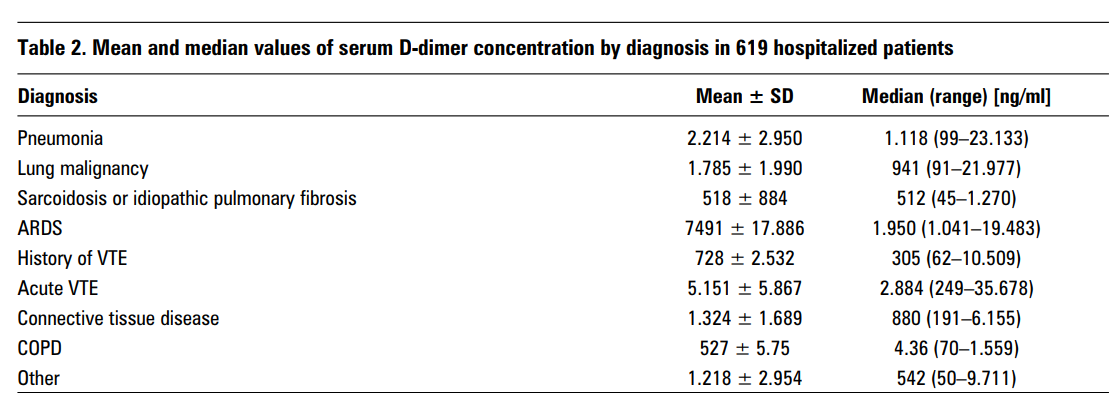
Ranges for various lung conditions
The principal utility of measuring D Dimer is the high NPV of the test in the diagnosis of Deep Venous Thrombosis (DVT) in an appropriate clinical setting. The clinical (pretest) probability (Wells score) of DVT is determined by assessing multiple factors, such as recent or ongoing therapy for cancer, immobilization of the lower extremities, recent major surgeries, localized tenderness, edema, and history of previous DVT. Based on this score, the probability for developing DVT is categorized as low (unlikely to develop) or high (likely to develop).
Empowering every Laboratory
Transasia Bio-Medicals Ltd., India’s leading in-vitro diagnostic company has been at the forefront of offering quality diagnostic solutions at a reasonable cost. In over three decades of its existence, Transasia has regularly introduced innovative and advanced technology based on the requirements of the customers.
ERBA ECL 105 and ECL 412 the latest semi-automated coagulation analyzers from Transasia are equipped to perform the D Dimer assay. Its affordability and easy availability, ensures that every laboratory can perform this test.
References:
- Aujesky, D., Roy, P.M., Guy, M., Cornuz, J., Sanchez, O. & Perrier, A.(2006) Prognostic value of D-dimer in patients with pulmonaryembolism. Thrombosis and Haemostasis, 96, 478–482.
- Carson, J.L., Kelley, M.A., Duff, A., Weg, J.G., Fulkerson, W.J.,Palevsky, H.I., Schwartz, J.S., Thompson, B.T., Popovich, Jr, J.,Hobbins, T.E., Spera, M.A., Alavi, A. &Terrin, M.L. (1992) Theclinical course of pulmonary embolism. New England Journal ofMedicine, 326, 1240–1245
- *http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/cardiology/venous-thromboembolism/Default.htm)
- **http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2873781/
- ***http://www.nmji.in/archives/Volume-23/Issue-4/PDF-volume-23-issue-4/Editorial.pdf
- ****http://www.japi.org/january2007/R-49.htm
- *****http://www.ncbi.nlm.nih.gov/pubmed/18160596